|
Auscultation of heart sounds
and murmurs R.
Beňačka, MD, PhD Aim: To gain basic
practical experiences and theoretical knowledge in auscultation of heart
sounds and murmurs in preclinical training.
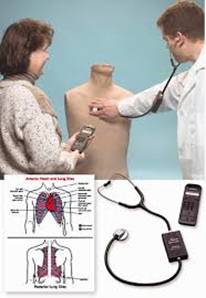
Methods: 1) For training of auscultations
skills the model simulator is used (The Life / Form Auscultation Trainer and
Smartscope simulator. The system is equipped with a the torso of the
chest of an adult man figurine,
wireless programmable unite containing with a set of pre-programmable
respiratory and cardiac sound phenomena and special stethoscope with sound
generator producing sounds in a stethoscope bell. When the bell is being moved over the
particular auscultatory points, the place – specific sounds are heard. A map
showing these typical auscultatory sites for both respiratory and cardiac
sounds is also available with the simulator and is of beneficial use. The
points are also noted by colors spots on the surface of figurine in order to
help in navigation. If the stethoscope bell is placed outside the usual
auscultation points no sound can be heard.
2) Students perform listening in within groups one after another. In
the beginning the auscultation for one or more sounds is demonstrated by the
teacher. After setting of the sound in program unite teacher uses stethoscope
to hear the sounds when mover over
specific points on figurine while students can hear the sounds through the
speaker. After then, each trial being
separated by sufficient disinfection of the olives in the stethoscope,
students can train listening of selected phenomena themselves. ---------------------------------------------------- Life/Form Auscultation
Trainer and Smartscope. (adult) (adult) Nasco (Fort Atkinson, Wisconsin): Lung: 5 anterior, 10
posterior, and 2 midaxillary locations. Heart: 6 anterior sites. Remote
controller selects heart and lung sounds. Smartscope plays sounds through
in-stelhoscope transceiver. Placement of stethoscope on chest activates
transponder playback of audio files. Dual headsets and remote speaker playback
options. |
|||||||||||
|
Heart auscultatory simulator 1 Normal sounds 2 Pulmonary stenosis 3 Aortic stenosis 4 Aortic regurgitation 5 Mitral stenosis 6 Mitral valve prolapse 7 Holosystolic (mitral regurgitation) 8 Midsystolic ejection 9 Midsystolic click 10 S3 Galop 11 S4 Gallop 12 Ventricular septal defect 13 Atrial septal defect pulm 14 Atrial septal defect int 15
Patent ductus arteriodus |
|
|
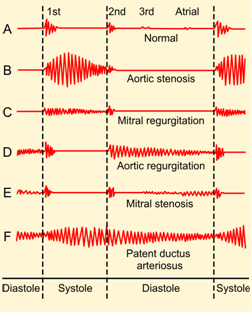
S1 = closure of tricuspidal and
mitral valves S2 = closure of aortic and pumonary artery valves (A)Systolic
murmus = after S1
(beween S1 and S2) –
Aortic stenosis/ Pulmonary stenosis –
Mitral regurgitation / Tricuspidal regurgitation –
Mitral valve prolaps (B)
Diastolic murmus =
after S2 (between S2 and S1) –
Aortic regurgitation/ Pulmonary regurgitation –
Mitral stenosis/ Tricuspidal stenosis (C)
Continuous murmurs Left
side problems (aortic, mitral) are much more common than right side defects. |
||||||||
|
|
|
|
|
||||||||
|
Murmur accoridng to duration Ø Systolic (after S1, between S1 & S2) -
Ejection -
Regurgitation Ø Diastolic (za S2, medzi S2 a S1) |
Phase of the heart cycle Ø Early (protosystolic, protodiastolic) Ø Medium (mezo-) Ø Late (tele-) Intensity change |
Change in intensity Ø Permanent (no change| Ø Crescendo Ø Decrescendous Ø Crescendo-descrescend |
Frequency of murmurs Ø Low frequency (murmur is called rumble) Ø Medium frequency (murmurs rough, coarse) Ø High frequency (blowing, vibrant| |
||||||||
|
The intensity of the murmur 1/6 minimum (for experienced) 2/6 quietest (hear when concentrating) 3/6 noisy (clear) 4/6 accompanied by palpable vortex 5/6 can also be heard with the edge of the
stethoscope 6/6 also in the stethoscope above the
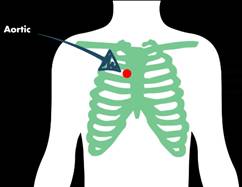
surface Where to hear ? Auscultation
sites: Ø Aortic point = 2nd intercostal space;
right to sternum Ø Pulmonic = 2nd intercostal space on
left to sternum Ø Tricuspid = 4th
intercostal space left close to sternum Ø Mitral = 4-5th intercostal space,
left over heart apex Ø Erb point = 3rd-intercostal
space; left from sternum |
Normal heartbeat sound consists of an S1 and an S2 and is heard
throughout the precordium It occurs without any rubs, gallops or murmurs. |
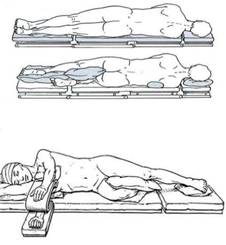
Decubital
posisiton
|
|||||||||
|
|
|||||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
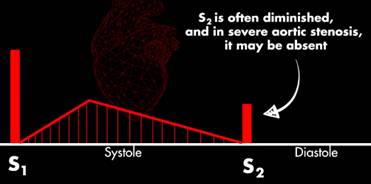
Aortic stenosis is a harsh crescendo – decrescendo systolic
ejection murmur and can be Listen: aortic point (right sternal boarder 2nd IC space);
radiates to the carotids. Pulsus
parvus et tardus (pulse weak and delayed) Cause: calcified aortic valves |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
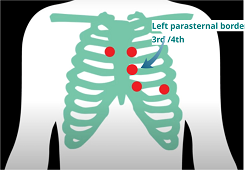
Aortic regurgitation (aortic insufficiency), is an early
diastolic decrescendo murmur .It is accompanied by wide pulse pressure Listen: aortic point (2nd IC space on left or even lower to left parasternal border at 3rd
and 4th IC space. Cause: bicuspid aortic valve defect ( endocarditis,
rheumatic fever, aortic valve base dilation (syphilitic aortitis) |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
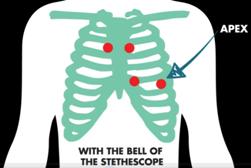
Mitral stenosis is a decrescendo-crescendo diastolic rumbling
murmur with loud S I click
(caused by the rapid closing of the thickened mitral valves) early diastolic opening snap ('snapping'
pf valve leaflets into the left
ventricle) following the opening snap
low-pitched diastolic murmur. It becomes louder - after a Valsalva maneuver after
exercise (increase afterload) Listen: apex Cause: rheumatic fever, heart valve calcification |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
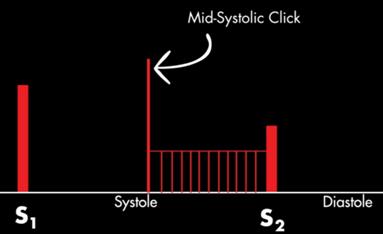
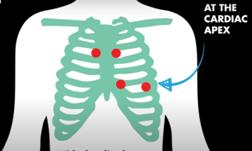
Mitral Valve Prolapse produces a mid-systolic click 'click'
made by a floppy leaflet snapping into a taut) followed by late systolic murmur due to backflow of blood during systole
from left ventricle to atrium. Most patients are asymptomatic. Palpitations
or chest pain may occur commonly. Complications of MVP include: arrhythmias
heart failure endocarditis Listen: best
in 5th IS mid-clavicular line;
in patient in left letral decubitus position Cause: Myxomatous degeneration of the mitral valve leaflets; MVP is present in
2% of population |
|
|
|||||||||
|
|
|
||||||||||
|
Mitral regurgitation is a holosystolic (pansystolic) murmur. When
the murmur begins after S1, it always continues to the 2nd heart sound (S2). Listen: heard best at the apex with the diaphragm of the stethoscope when the
patient is in the left lateral decubitus position. |
|||||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
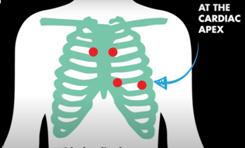
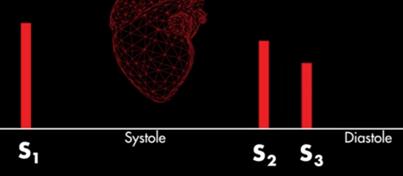
S3 Heart Sound is a low pitch sound produced by blood
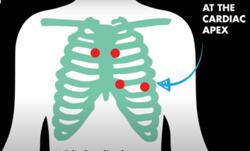
coming into contact with compliant ventricle after S2 click. Listen: cardiac apex; in the left lateral decubitus position Cause:
In adults or elderly persons S3 is pathological. Normally present: Young
adults, children. pregnancy, athletes, severe mitral & tricuspidal
regurgitation, cardiomyopathy, heart failure |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
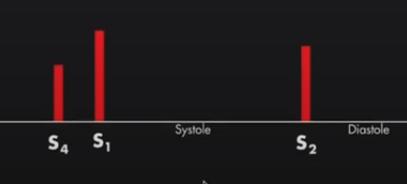
S4 Heart Sound (aka "atrial
gallop") is late diastolic low-frequency heart sound
occurring prior to S1m during the
atrial filling phase in diastole and coincides with P in ECG (atrial
systole). Listen: cardiac apex; in the left lateral decubitus position Cause: turbulence
as blood enters a stiff ventricle. |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
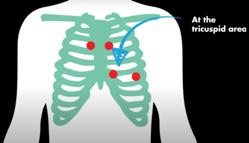
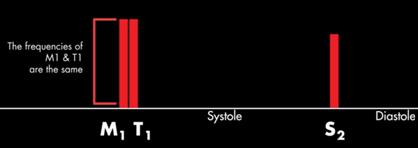
Split S1 means that separate clicks M1 and T1 are heard
instead of S1 (simultaneous closure of
the tricuspid and mitral values). M1 andT1 sound the same. Listen:
tricuspidal area Cause: It is normal finding; can be heard in app.
40 - 70% of adults; Also it be heard in Right Bundle Branch Block (RBBB).when
LV is depolarized earlier than RV. This cause that MV and TV start differently. !
Differentiate split S 1 from
pathologic S4.(sounds in lower frequency than S1) |
|
|
|||||||||
|
|
|
|
|||||||||
|
|
|
|
|||||||||
|
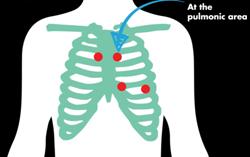
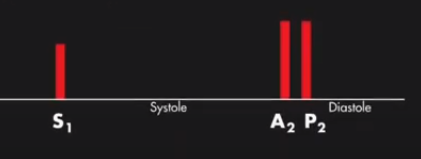
Split S2 means
that separate clicks A2 and P2 are heard instead of S2 (simultaneous closure
of the aortic and pulmonic valves). Valves close at different times. A2
occurs normally before P2, in pathol,
cases P2 occurs before A2. Listen: pulmonic area Cause: In a normal person, heart
alternates between single S2 & split S2 sound during inspiration;
Pathology: Pulmonic
stenosis (wide split S2), Right bundle branch blocks |
|
|
|||||||||
|
S2
split can be exaggerated by deep inspiration,
which causes an increased venous return to the right side of the
heart leading to the delayed closure of the pulmonic valve.
Compared to a S3, which is heard later in the cycle, the split S2 heart
sounds are higher in pitch vs.the S3 which is typically lower in pitch Fixed
Split S2 (persistent split S2): Atrial septal defects, Pulmonary
Hypertension, Right heart failure Paradoxical
S2 (P2 before A2): Aortic stenosis, Right Venticular
pacemaker, Left bundle branch block |
|||||||||||
|
|
|
||||||||||
|
|
|
||||||||||
|
Pediatric murmus |
|
||||||||||
|
An innocent murmur is the sound(s) created by
the vibrations of the heart walls as the blood flows through the chambers and
valves. They are harmless. These are are of systolic murmurs of short duration low intensity, grade 1-2
/ 6, They often occur in children (80%) and disappear in adulthood. They do
not require any treatment. |
|||||||||||
|
|
|
|
|||||||||
|
Still's murmur is a long-lasting but pronounced
low-frequency vibrational murmur (similar to string vortexing) that occurs
during auscultation at the lower edge of the sternum, most common in
preschool children and toddlers. It changes with position and it is best to
hear the recliners. Its intensity increases after exertion and weakens during
the Valsava maneuver. |
|||||||||||
|
|
|
|
|||||||||
|
The physiological ejection
murmur above
the pulmonary artery is the systolic mumur that is most heard in the 2nd
intercostal space on left ti the sternum (P point). It is more common in
schoolchildren and adolescents. It can be confused with ausculatory findings
in mild pulmonary stenosis or a defect of the atrial septum. Here, normal
finding of S2 above the lungs (without split or clicks) is important |
|||||||||||



|
Recommended audiovisual
internet resources A) Heart auscultation MEDZCOLL collection ·
Normal
Heart Sounds: https://youtu.be/FtXNnmifbhE ·
Aortic
Stenosis: https://youtu.be/pgDWz1JybzE ·
Aortic
Regurgitation: https://youtu.be/uZysrKXHJMM ·
Mitral
Valve Prolapse: https://youtu.be/sH_KmHIHR70 ·
Mitral
Stenosis: https://youtu.be/5oCPtZo4pUY · |
·
Split
S1 Heart Sounds: https://youtu.be/kvQ2IU3ILRo ·
Split
S2 Heart Sound: https://youtu.be/98HM1fr3cq4 ·
S3
Heart Sound: https://youtu.be/_i2D1KZkN1w ·
S4
Heart Sound: https://youtu.be/KcMF8rJDTIk ·
S3
and S4 Gallop: https://youtu.be/o8eqYHCy7dw ·
Innocent
Murmur - https://youtu.be/uFyWHPfrRak |
|
|
|
B)
Other collection
|
Heart Sounds and Heart Murmurs, Animation: https://www.youtube.com/watch?v=dBwr2GZCmQM |
|
|
|
|
|
|
|
|
|
Heart Murmurs and Heart Sounds: Visual
Explanation for Students https://www.youtube.com/watch?v=wYZbMoWjLEg |
|
|
|
|
|
|
|
|
|
http://depts.washington.edu/physdx/heart/demo.html |
|
|
|
|
|
|
|
|
|
Acute Coronary Syndrome: Unstable Angina,
NSTEMI and STEMI https://www.youtube.com/watch?v=C0BUPHYQ1h4 |
|
|
|
|
|
|
|
|
|
Systolic
murmurs, diastolic murmurs, and extra heart sounds - Part 1 | NCLEX-RN | Khan
Academy Systolic
murmurs, diastolic murmurs, and extra heart sounds - Part 1 | NCLEX-RN | Khan
Academy https://www.youtube.com/watch?v=ZUHpAaVpiY8 |
|
|
|
|
|
|
|




